Table of contents
Dr. Gregor's Grand Rounds Video
The Modern Metabolic Pandemic: How DNA, Diet and Destiny Collide
The Core Problem: A Global Metabolic Collapse
Across continents, the same pattern is emerging: obesity, fatty liver disease, type 2 diabetes, hypertension, chronic kidney disease, and cardiovascular disease. These are not separate epidemics. They are one metabolic disorder expressing itself through multiple organs. The unifying mechanism is metabolic overload — a mismatch between human biology and the modern food environment.
The Central Mechanism: Fructose Overload
Fructose is the biochemical accelerant of the modern metabolic crisis. It is metabolized almost entirely in the liver. It generates uric acid, fat, and oxidative stress. It suppresses ATP, triggering hunger and fat storage. It overwhelms mitochondria. It drives hepatic insulin resistance, the root of metabolic syndrome. This is not a calorie problem. It is a biochemical problem.
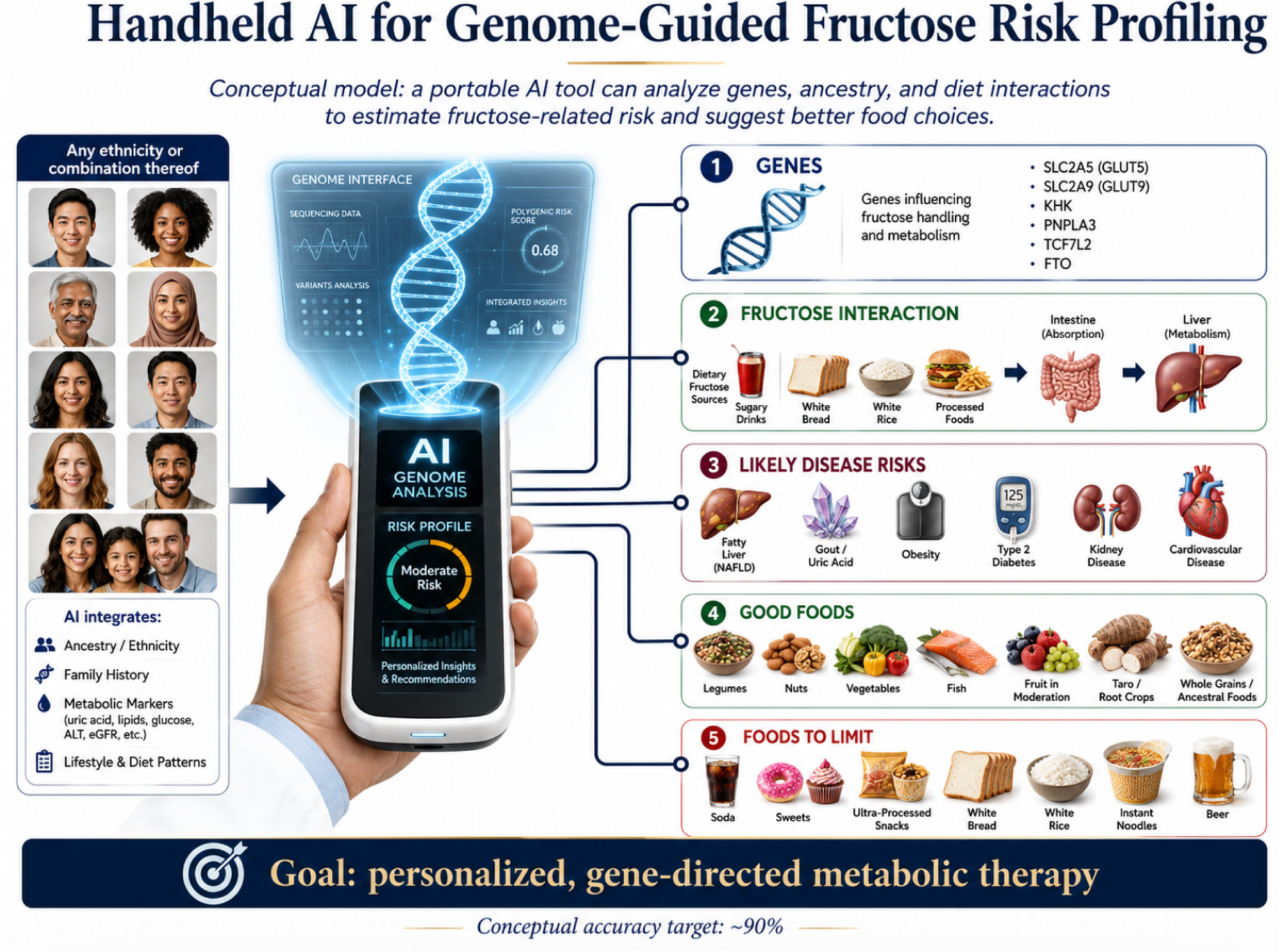
The Hidden Accelerator: Genetic Vulnerability
Genes load the gun. The modern diet pulls the trigger. Populations with thrifty genotypes, uricase pathway mutations, ancestral famine exposure, rapid dietary modernization, or migration from low‑sugar to high‑sugar environments experience catastrophic metabolic deterioration when exposed to Westernized diets. This explains the disproportionate burden of metabolic disease in Pacific Islanders, Indigenous peoples, South Asians, Latin American populations, and African diaspora communities. Destiny is not fixed — but risk is inherited.
The Perfect Storm: Food Systems vs. Human Biology
Modern food systems are engineered for hyper‑palatability, ultra‑processing, high fructose content, low cost, and addictive reward pathways. This creates a biological mismatch between ancient genes and modern diets. The result is predictable: a global metabolic pandemic.
The Clinical Cascade: From Liver to Lifespan
Fructose overload triggers a multi‑organ cascade.
Liver: de novo lipogenesis, NAFLD to NASH, hepatic insulin resistance.
Pancreas: hyperinsulinemia, beta‑cell stress.
Kidneys: uric acid–mediated injury, hypertension.
Vasculature: endothelial dysfunction, atherosclerosis.
Brain: appetite dysregulation, reward pathway hijacking.
Metabolic disease is not a willpower issue. It is a systemic biochemical disorder.
The Clinical Message: Diet Must Match DNA
Personalized nutrition is essential, not optional. Patients need diets aligned with genetic ancestry, metabolic phenotype, uric acid sensitivity, mitochondrial resilience, insulin response, and liver fat burden. This is the future of preventive medicine.
This Grand Rounds summary distills decades of clinical observation, biochemical analysis, and global public health insight into a framework that empowers individuals and communities to reclaim metabolic health.
Comments from Dr Carlos Monteiro: "I just watched, wonderful.", Carlos Carlos A. Monteiro MD, PhD Emeritus Professor, School of Public Health,University of Sao Paulo
Comments from Dr Richard J Johnson: "Hi. I just watched your talk- bravo! I am glad you realize how important fructose and uric acid are. I have hope that one day we can replace the uricase gene in humans. Congratulations again on all of your work and effort"
Comments from Dr Dean Winslow: "Great talk, Peter! " Dean Dean L. Winslow, MD, MACP, FRCP(Lon), FAAP, FIDSA, FPIDS, Professor of Medicine, Division of Infectious Diseases and Geographic Medicine, Stanford University School of Medicine