Uric Acid, Fructose, Gout, Hypertension, and Kidney Disease
Introduction
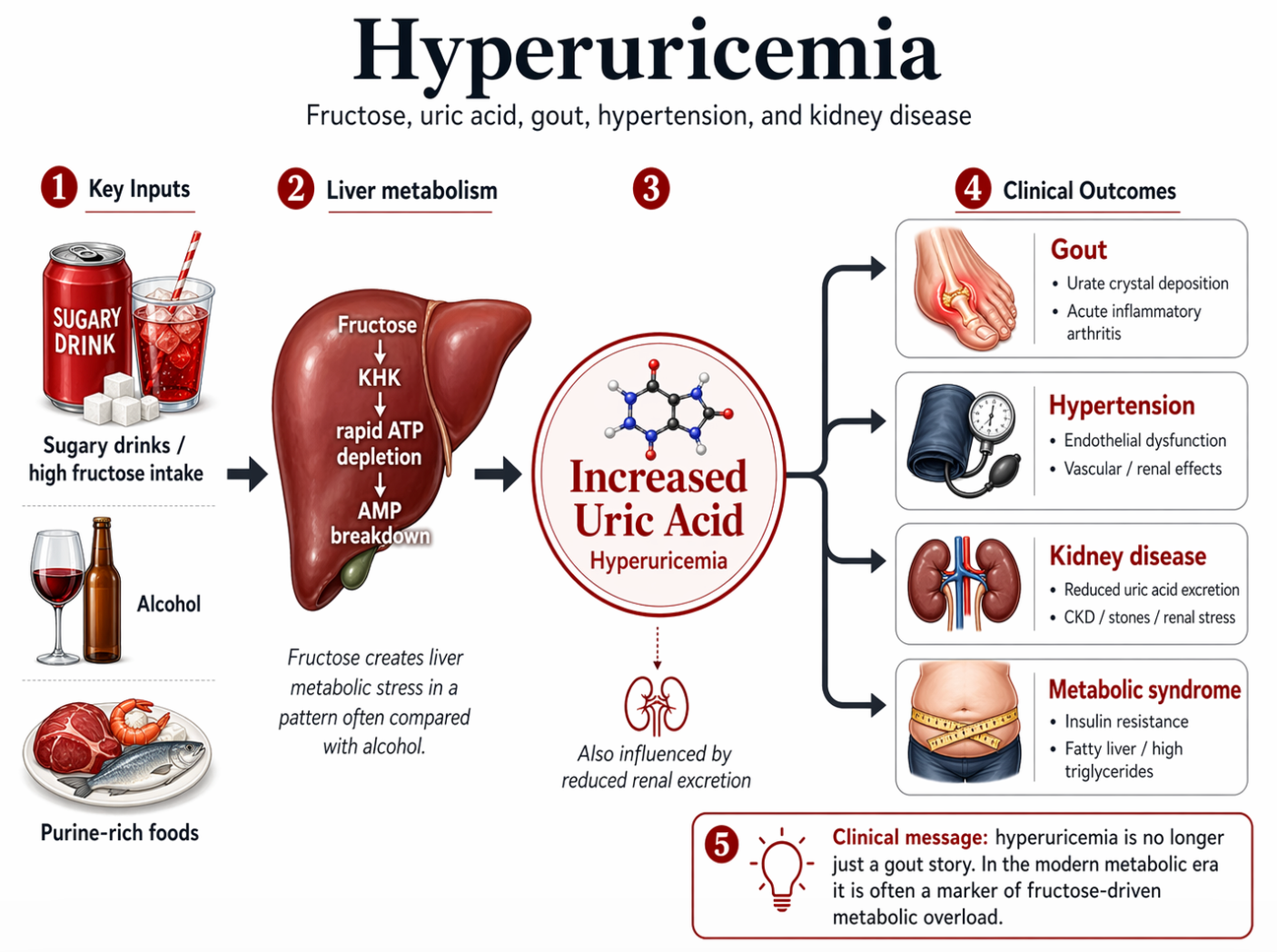
Hyperuricemia means an elevated level of uric acid in the blood.
For many years, uric acid was discussed mainly in relation to gout, shellfish, purines, and alcohol. That clinical picture is still important, but it is no longer the whole story.
In the modern metabolic era, hyperuricemia is also strongly linked to:
- fructose intake
- insulin resistance
- metabolic syndrome
- hypertension
- chronic kidney disease
- fatty liver disease
This matters because uric acid is not simply a bystander. In many patients, it is a clinical marker of metabolic overload and may also contribute directly to disease. Uric acid sits near the center of the fructose--ATP depletion– insulin resistance pathway and deserves routine attention in metabolic evaluation, especially where gout, fatty liver, hypertension, diabetes and chroinic kidney disease cluster together.
What is uric acid?
Uric acid is the end product of purine metabolism in humans.
Purines come from:
- normal turnover of the body’s own cells
- certain foods
- alcohol-related metabolic stress
- fructose-driven ATP depletion in the liver
Normally, uric acid is filtered and excreted largely by the kidneys, with some handling through the gut.
When production rises or excretion falls, serum uric acid increases.
Hyperuricemia is no longer just a “gout story”
The old clinical teaching emphasized:
- red meat
- shellfish
- organ meats
- alcohol
- purine-rich foods
Those still matter, especially in classic gout.
But today, many patients with hyperuricemia also have a broader metabolic pattern:
- central obesity
- elevated triglycerides
- prediabetes or diabetes
- hypertension
- fatty liver
- reduced kidney function
This is why hyperuricemia increasingly belongs in the same conversation as metabolic syndrome.
The fructose connection
One of the most important modern drivers of hyperuricemia is fructose.
Fructose is handled differently from glucose. It is metabolized primarily in the liver, where it is rapidly phosphorylated by ketohexokinase (KHK). This rapid process can:
- consume ATP
- generate AMP breakdown products
- increase uric acid production
- promote de novo lipogenesis
- increase triglycerides
- worsen insulin resistance
This is one reason fructose has often been described as behaving “like alcohol in the liver.”
That does not mean fructose and alcohol are identical substances. It means they share important metabolic features:
- both are handled heavily by the liver
- both can promote fat production in the liver
- both can increase metabolic stress
- both can increase uric acid generation
This makes fructose particularly important in the clinical story of hyperuricemia.
Why sugary drinks matter
Hyperuricemia is especially linked to liquid fructose exposure, including:
- soft drinks
- sugar-sweetened beverages
- sweetened juices
- energy drinks
- high-sugar processed beverages
These are clinically important because they deliver fructose:
- rapidly
- in large quantity
- with little satiety
- without the fiber of whole fruit
This creates a pattern of repeated liver exposure that can drive both uric acid and fatty liver.
Hyperuricemia and gout
The most familiar clinical syndrome associated with hyperuricemia is gout.
Gout occurs when monosodium urate crystals deposit in joints and trigger intense inflammation.
Typical features include:
- sudden severe joint pain
- redness and swelling
- tenderness
- recurrent attacks
- common involvement of the first metatarsophalangeal joint (the great toe), but also ankles, knees, wrists, and other joints
Not everyone with hyperuricemia develops gout, but elevated uric acid increases risk.
Traditional gout triggers
Classic triggers still matter:
- alcohol
- dehydration
- purine-rich foods
- shellfish
- organ meats
- some medications, especially diuretics
Tomatoes are sometimes reported by patients as a trigger, but they are not the central metabolic story. In the modern setting, the broader driver is often fructose exposure plus metabolic dysfunction.
Hyperuricemia and hypertension
Hyperuricemia is also linked to hypertension.
Several mechanisms have been proposed, including:
- endothelial dysfunction
- oxidative stress
- impaired nitric oxide signaling
- renal microvascular effects
- activation of sodium-retaining and vasoconstrictive pathways
Clinically, many patients with elevated uric acid also have:
- high blood pressure
- central obesity
- insulin resistance
- elevated triglycerides
Hyperuricemia and the aortic wall.
Emerging evidence suggests that elevated serum uric acid is associated with aortic aneurysm disease and may contribute to aortic wall vulnerability through oxidative stress, endothelial dysfunction, vascular inflammation, smooth-muscle injury, and matrix degradation.
A large Japanese cohort found hyperuricemia to be an independent predictor of death from aortic disease, including dissection and ruptured aneurysm, while a Mendelian randomization study supported a causal association with aortic aneurysm risk but not clearly with dissection itself. The best current interpretation is that uric acid is not simply “crystals scraping the artery,” but a metabolic-inflammatory signal that may weaken the aortic wall over time, especially in the presence of hypertension, kidney disease, insulin resistance, and other cardiometabolic stressors.
References:
Otaki Y, Watanabe T, Konta T, et al. Impact of hyperuricemia on mortality related to aortic diseases: a 3.8-year nationwide community-based cohort study. Scientific Reports. 2020;10:14281.
Lin ZP, He HQ, Aierken Y, Wu Y, Liu Y. Effect of serum uric acid on the risk of aortic aneurysm and dissection: A Mendelian randomization analysis. Biochemistry and Biophysics Reports. 2024;38:101743.
This does not mean every case of hypertension is caused by uric acid. It means hyperuricemia is often part of the same cardiometabolic cluster.
Hyperuricemia and kidney disease
The kidneys play a central role in uric acid handling, so hyperuricemia and kidney disease often reinforce one another.
Kidney-related consequences include:
- reduced uric acid excretion as kidney function declines
- worsening hyperuricemia in chronic kidney disease
- uric acid kidney stones in some patients
- possible contribution to renal vascular and interstitial injury
This creates a clinical loop:
kidney dysfunction → less uric acid excretion → higher uric acid
and possibly
higher uric acid → more renal stress
In patients with chronic kidney disease, elevated uric acid should not be dismissed as an isolated laboratory abnormality. It may be a marker of broader metabolic and renal stress.
Hyperuricemia and metabolic syndrome
Hyperuricemia frequently appears alongside:
- abdominal obesity
- insulin resistance
- elevated fasting glucose
- elevated triglycerides
- low HDL
- hypertension
- fatty liver disease
That is why serum uric acid can be viewed as a red flag in metabolic evaluation.
It does not replace other markers, but it often helps identify patients whose metabolic disease is more advanced than it first appears.
Hyperuricemia and fatty liver
Fructose links uric acid and liver disease in a clinically important way.
Excess fructose intake can lead to:
- ATP depletion
- uric acid generation
- hepatic fat accumulation
- elevated triglycerides
- worsening insulin resistance
This means patients with hyperuricemia may also have:
- MASLD
- elevated liver enzymes
- central adiposity
- hypertriglyceridemia
In that sense, hyperuricemia is often not just a crystal problem. It is part of a larger liver-centered metabolic pattern.
When to think clinically about hyperuricemia
Hyperuricemia becomes especially relevant when it appears in a patient with:
- recurrent gout
- hypertension
- chronic kidney disease
- obesity
- prediabetes or diabetes
- fatty liver disease
- high sugar or sugary beverage intake
- elevated triglycerides
In such patients, uric acid is often helping tell a broader metabolic story.
Clinical presentation
Patients with hyperuricemia may present in several ways:
1. Asymptomatic hyperuricemia
- elevated uric acid on blood testing
- no gout symptoms yet
- often found during metabolic evaluation
2. Gout
- acute painful inflammatory arthritis
- recurrent flares
- possible tophi in chronic disease
3. Kidney manifestations
- nephrolithiasis
- chronic kidney disease
- worsening renal function
4. Metabolic clustering
- hypertension
- central obesity
- insulin resistance
- fatty liver
- dyslipidemia
Clinical Perspective
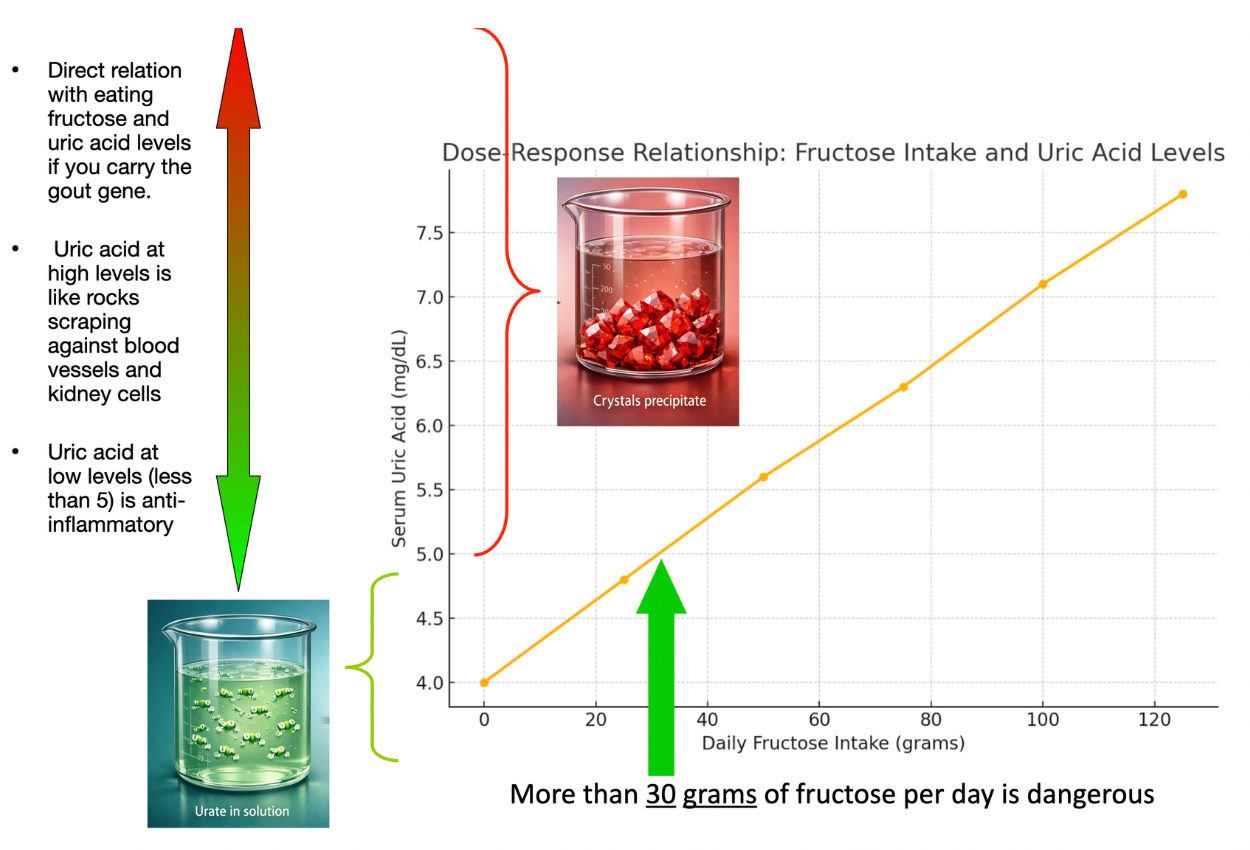
In clinical practice, elevated uric acid is most commonly associated with gout. However, its relationship to metabolic disease has prompted broader interest in measuring uric acid levels as part of metabolic evaluation. One hundred years ago the average uric acid in humans level was 4. Now it is 5. Perhaps the rise in the average uric acid level in humans over the past hundred years tells us something about the increasing fructose content of the 21st Century diet.
Some clinicians view elevated uric acid as a potential marker of metabolic stress, particularly when it appears alongside other indicators such as insulin resistance, elevated triglycerides, or fatty liver disease.
Further research is continuing to clarify its role in metabolic physiology.
A more modern clinical view
The research from Lustig's group at the University of Caslifonia San Francisco (UCSF) established that fructose behaves like alcohol in hte liver. Therefore, if a sugar sweetened beverage loaded with frucotse contains 20 grams of fructose, and a can of beer contains twenty grams of fructose, they are both considered as fructose laden sources of the precursors of uric acid.
On Saipan, Dr Gregor has seen two young patients develop extremely high uric acid levels from drinking 4 "regular" sodas every day for three years. From the hyperuricemia, both are now on dialysis.
A modern clinical approach to hyperuricemia should consider not just the 2oth century "causes" but now with the high probability of fructose in the diet causing elevation in uric acid levels in a manner similar to beer. A 21st Century clinician should consider 2 questions:
Question 1
Is this patient at risk for crystal disease?
- gout
- tophi
- uric acid stones
- genetic predisposition for distorted GLUT9 metabolism, e.g. Pacific Islander?
Question 2
Is this patient showing signs of metabolic overload?
- high fructose intake (beer, sodas, white rice, white processed breads)
- fatty liver
- insulin resistance
- hypertension
- chronic kidney disease
- unknown uric acid level
This broader view is important because focusing only on purines may miss an important driver in many modern patients, specifically added fructose in the food.
Practical lifestyle considerations
In patients with hyperuricemia, useful clinical counseling may include:
- reduce sugar-sweetened beverages
- reduce high-fructose processed foods
- moderate or avoid alcohol, especially beer and spirits when relevant
- address weight gain and visceral adiposity
- improve overall dietary pattern
- maintain hydration
- review medications that may raise uric acid
Traditional purine counseling still has a role, but in the metabolic era it should often be combined with a clear discussion of fructose.
Bottom line
Hyperuricemia is no longer just a story about gout, shellfish, and alcohol.
In the modern food environment, it is often part of a broader pattern involving:
- fructose exposure
- liver metabolic stress
- insulin resistance
- hypertension
- kidney disease
- metabolic syndrome
Fructose is especially important because it is metabolized in the liver in a way that promotes:
- ATP depletion
- uric acid generation
- liver fat
- triglyceride production
In many patients, elevated uric acid is therefore both:
- a clue to gout risk
- and a clue to underlying metabolic disease