Kidney Dysfunction in the Cardiometabolic Era
Introduction
“Renal failure” is often used broadly in public discussion, but clinically it usually refers to advanced kidney dysfunction, often within the larger spectrum of chronic kidney disease (CKD). KDIGO defines CKD as abnormalities of kidney structure or function present for more than 3 months with implications for health, and classifies it by cause, GFR category, and albuminuria category.
In modern clinical practice, kidney disease is rarely an isolated organ problem. It is deeply connected to obesity, diabetes, hypertension, fatty liver disease, and cardiovascular disease. The American Heart Association now explicitly frames these connections within cardiovascular-kidney-metabolic (CKM) syndrome, recognizing that the heart, kidneys, metabolism, and adipose tissue are biologically intertwined.
For your site, renal failure belongs squarely in the metabolic disease section because many modern cases arise in the setting of chronic metabolic overload.
What the kidneys do
The kidneys are not just filters.
They regulate:
- fluid balance
- sodium and potassium balance
- acid-base balance
- blood pressure
- waste excretion
- endocrine functions such as erythropoietin and vitamin D activation
When kidney function declines, the consequences spread well beyond the kidneys themselves.
From chronic kidney disease to renal failure
Kidney disease usually progresses through stages.
At first, damage may appear as:
- albuminuria
- a decline in estimated glomerular filtration rate (eGFR)
- structural kidney abnormalities
Over time, some patients progress to kidney failure, generally corresponding to G5 CKD, when eGFR falls below 15 mL/min/1.73 m² or kidney replacement therapy becomes necessary.
So “renal failure” is often the late expression of a much longer disease process.
Why kidney disease belongs to metabolic syndrome
Kidney disease is closely linked to the same metabolic disturbances that drive:
- Type 2 diabetes
- hypertension
- fatty liver disease
- visceral obesity
- cardiovascular disease
This is why CKD fits so naturally inside the framework of metabolic syndrome and CKM syndrome. The AHA’s 2023 scientific statement emphasizes that obesity, diabetes, CKD, and cardiovascular disease are not separate silos but part of one connected health disorder.
Diabetes and kidney damage
Type 2 diabetes remains one of the most important causes of chronic kidney disease.
Persistent hyperglycemia can injure the kidney’s microvasculature and filtration system, leading over time to:
- albuminuria
- declining GFR
- progressive nephropathy
- eventual kidney failure in some patients
This is one reason kidney disease should not be thought of as a separate condition appearing after diabetes. In many patients, it is part of the same metabolic trajectory.
👉 See: Type 2 Diabetes
Hypertension and the kidney
Hypertension is both a cause and a consequence of kidney disease.
Elevated blood pressure can damage small vessels in the kidney, impairing blood flow and filtration. As kidney function worsens, sodium and fluid handling become abnormal, which can further raise blood pressure.
This creates a vicious cycle:
hypertension → kidney injury → worsening blood pressure control
That is why kidney disease, metabolic syndrome, and hypertension are so tightly linked in clinical practice.
👉 See: Hypertension
Obesity, visceral adiposity, and kidney risk
Excess adiposity—especially visceral fat—is increasingly recognized as an upstream driver of kidney disease.
Visceral fat contributes to:
- insulin resistance
- inflammatory signaling
- altered kidney hemodynamics
- activation of sodium-retaining and pressure-raising pathways
This means that kidney disease in many patients begins not only with diabetes or hypertension, but with adiposity-driven metabolic dysfunction.
👉 See: Visceral Obesity
The liver–kidney connection
One of the most important modern themes is the overlap between kidney disease and fatty liver disease (MASLD).
Recent reviews note that CKD is more common in patients with MASLD and that risk rises further in more advanced steatotic liver disease. Several 2025 reviews and meta-analytic studies support a significant association between steatotic liver disease and CKD risk, even if questions remain about causality in every case.
This matters because it links the kidney directly to the same metabolic environment that drives:
- hepatic fat accumulation
- insulin resistance
- elevated triglycerides
- chronic inflammation
In many patients, kidney disease is therefore part of a broader hepato-metabolic syndrome.
👉 See: Fatty Liver Disease (MASLD)
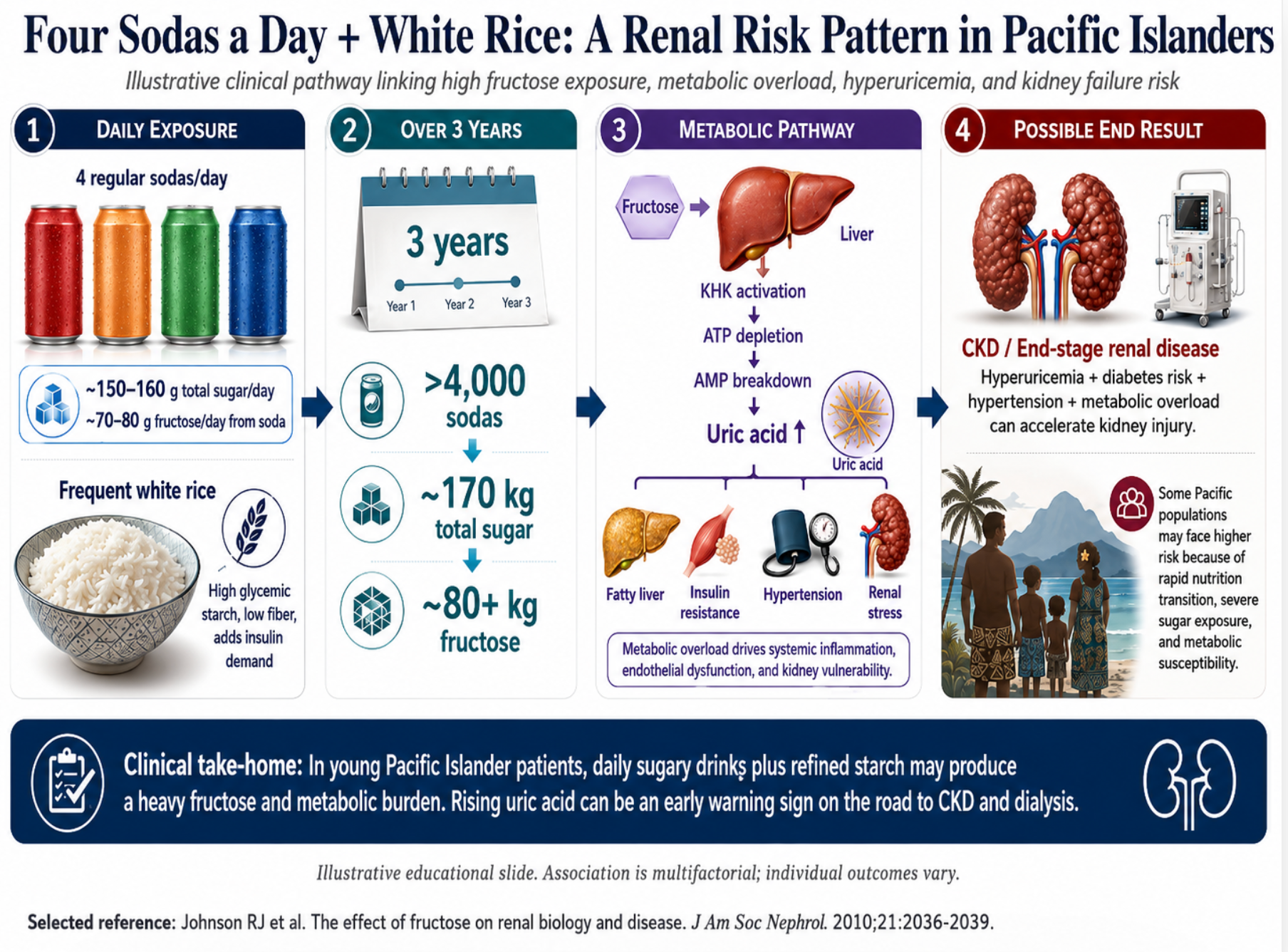
Fructose and the kidney
Fructose is not the sole cause of kidney disease, and not all renal failure is fructose-related. But in the modern food environment, fructose is clinically relevant because it can contribute to several upstream processes that burden the kidney.
High fructose exposure can promote:
- ATP depletion in the liver
- uric acid generation
- insulin resistance
- fatty liver
- elevated triglycerides
- hypertension
These changes may indirectly worsen renal risk through metabolic overload, vascular dysfunction, and blood-pressure elevation. Experimental and epidemiologic work increasingly supports the idea that fructose-associated uric acid may contribute to kidney injury in some settings.
👉 See: Fructose Metabolism
👉 See: Uric Acid
Uric acid and renal disease
Uric acid is especially important in kidney disease because the kidneys are the main route of uric acid excretion.
As kidney function declines:
- uric acid excretion falls
- serum uric acid rises
- hyperuricemia becomes more common
At the same time, hyperuricemia may contribute to:
- endothelial dysfunction
- renal vascular stress
- oxidative stress
- further decline in kidney health in susceptible patients
Recent reviews continue to describe hyperuricemia as strongly linked to CKD progression, though the exact degree of causality is still debated.
This makes hyperuricemia both:
- a consequence of kidney dysfunction
- and, in some patients, a possible amplifier of further injury
Inflammation and the kidney
Kidney disease in the metabolic era is not only about glucose and blood pressure. It is also about chronic low-grade inflammation.
Inflammatory signaling from:
- visceral adipose tissue
- the liver
- vascular endothelium
- altered gut-kidney pathways
may contribute to progressive renal dysfunction. Reviews of the kidney-gut axis in CKD have emphasized the growing recognition of systemic metabolic and inflammatory contributions to kidney disease.
This fits your broader framework: modern renal failure often sits at the intersection of metabolism, inflammation, and vascular biology.
Clinical presentation
Kidney disease can be silent for years.
Patients may first come to attention because of:
- abnormal serum creatinine
- reduced eGFR
- albumin in the urine
- resistant hypertension
- edema
- anemia
- electrolyte disturbance
In later disease, renal failure may lead to:
- fluid overload
- uremic symptoms
- severe hypertension
- worsening cardiovascular instability
- need for dialysis or transplantation
Why kidney disease is so dangerous
Kidney disease is dangerous not only because of loss of filtration, but because it amplifies risk across multiple systems.
CKD increases the risk of:
- cardiovascular disease
- heart failure
- arrhythmia
- stroke
- mortality
This is one reason the CKM model is so clinically useful: once the kidney becomes involved, the broader cardiometabolic syndrome often becomes more severe.
Treatment in the modern era
Modern kidney care increasingly requires treatment of the whole metabolic environment, not just kidney numbers.
This includes:
- aggressive blood pressure control
- diabetes management
- reduction of visceral adiposity
- improvement in diet quality
- reduction of sugary beverages and ultra-processed foods
- management of hyperuricemia where relevant
- evidence-based use of kidney-protective therapies such as SGLT2 inhibitors in appropriate patients
KDIGO 2024 places major emphasis on integrated risk reduction and holistic treatment rather than viewing CKD in isolation.
A broader metabolic interpretation
The most useful way to think about renal failure in many modern patients is this:
It is often not just a kidney disease.
It is the kidney expression of a broader disorder involving:
- metabolic syndrome
- insulin resistance
- visceral adiposity
- fatty liver
- hypertension
- cardiovascular disease
This perspective makes more sense clinically than treating renal failure as a late isolated endpoint.
Bottom line
Renal failure is often the late-stage outcome of chronic kidney disease, but in the modern era it frequently develops within a broader cardiovascular-kidney-metabolic syndrome.
For many patients, the underlying drivers include:
- diabetes
- hypertension
- obesity
- visceral fat
- fatty liver
- hyperuricemia
- high fructose and ultra-processed food exposure
Not every case follows this pathway, but in a large share of modern patients, renal failure is best understood as advanced metabolic disease expressed through the kidney.
Related pages
Metabolic Syndrome
Type 2 Diabetes
Hypertension
Hyperuricemia
Fatty Liver Disease (MASLD)
Fructose Metabolism
Uric Acid
Sleep Apnea
Cardiovascular Disease