Heart Failure With Preserved Ejection Fraction
Heart Failure With Preserved Ejection Fraction in the Cardiometabolic Era
Introduction
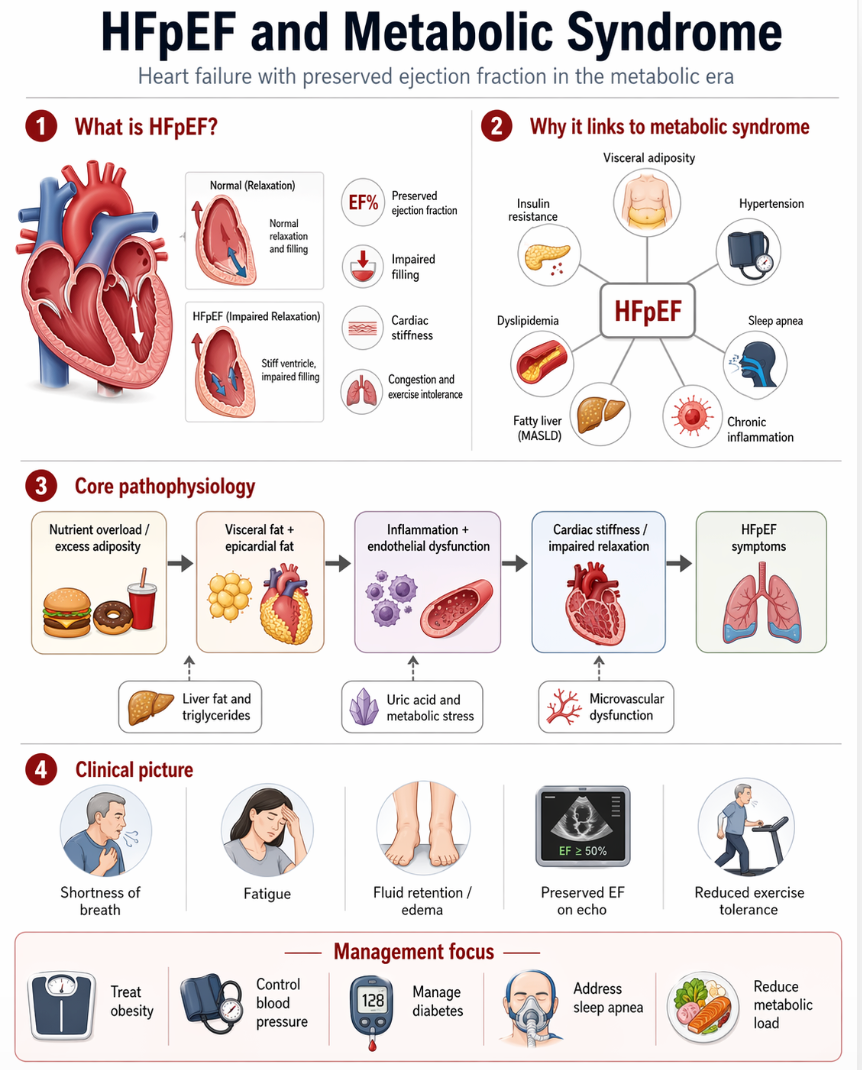
Heart failure with preserved ejection fraction (HFpEF) is now one of the dominant forms of heart failure in clinical practice. It is defined by the syndrome of heart failure in the setting of a left ventricular ejection fraction that is not reduced, usually with evidence of impaired ventricular relaxation, elevated filling pressures, left atrial remodeling, pulmonary congestion, and exercise intolerance. It is not a benign diagnosis and is associated with substantial morbidity, recurrent hospitalization, and mortality.
A modern clinical view of HFpEF is that it is often not a purely hemodynamic disorder. In many patients—especially those with obesity, diabetes, fatty liver disease, hypertension, sleep apnea, and chronic kidney disease—it is better understood as a multisystem cardiometabolic syndrome. Recent JACC work has gone even further, arguing that obesity-related HFpEF is, in many cases, an adiposity-driven disease in which visceral and epicardial fat, altered adipokine signaling, systemic inflammation, and metabolic overload shape the syndrome from the outset.
Clinical definition and diagnosis
HFpEF remains a clinical diagnosis. Patients typically present with:
- exertional dyspnea
- exercise intolerance
- edema or congestion
- fatigue
- elevated natriuretic peptides in many, though not all, cases
- echocardiographic evidence of preserved EF with structural and functional abnormalities such as left atrial enlargement, concentric remodeling, left ventricular hypertrophy, or diastolic dysfunction
No single test definitively establishes HFpEF in all patients. The diagnostic process relies on symptoms and signs of heart failure, preserved EF, objective evidence of elevated filling pressures or diastolic dysfunction, and careful exclusion of alternative explanations. ACC guidance emphasizes structured diagnostic assessment because HFpEF is frequently underrecognized and often mislabeled.
Why HFpEF belongs in metabolic disease
HFpEF overlaps heavily with:
- obesity
- metabolic syndrome
- Type 2 diabetes
- hypertension
- sleep apnea
- chronic kidney disease
- fatty liver disease
This clustering is not incidental. ACC’s 2023 expert consensus specifically places management of comorbidities at the center of HFpEF care, naming hypertension, obesity, diabetes, atrial fibrillation, and sleep apnea as primary treatment targets. In other words, HFpEF frequently sits downstream of the same biologic processes that drive broader metabolic disease.
Pathophysiology: beyond diastolic stiffness alone
The classic description of HFpEF emphasizes a stiff ventricle with impaired relaxation. That remains true, but contemporary research shows that the disorder extends beyond myocardial stiffness. Current models emphasize a network of abnormalities that may include:
- systemic inflammation
- endothelial and coronary microvascular dysfunction
- left ventricular hypertrophy and fibrosis
- plasma volume expansion
- skeletal muscle impairment
- renal dysfunction
- visceral and epicardial adiposity
In obesity-related HFpEF, these abnormalities appear to be tightly linked to dysfunctional adipose tissue biology. The 2025 JACC State-of-the-Art Review by Milton Packer proposes that visceral adiposity and altered adipokines are major upstream drivers of obesity-related HFpEF, offering a unifying framework for the syndrome.
Visceral adiposity and epicardial fat
A major advance in the field has been recognition that fat depots around and within the cardiometabolic system are not passive. Visceral adipose tissue contributes to inflammatory signaling, insulin resistance, and altered vascular regulation. Epicardial and paracardiac adipose tissue may be especially relevant in HFpEF because they lie adjacent to the myocardium and coronary microcirculation.
This matters clinically because obesity-related HFpEF is not just “heart failure in a heavier person.” It is often a disease in which abnormal fat distribution and dysfunctional fat biology contribute directly to symptoms, structure, and outcomes. Reviews and imaging studies have increasingly linked epicardial or paracardiac adiposity to myocardial stiffness, impaired exercise tolerance, and adverse remodeling.
The adipokine hypothesis
The adipokine hypothesis provides a particularly useful framework. In this model, hypertrophied visceral adipocytes become abnormal endocrine organs, releasing a maladaptive profile of signaling molecules that promote:
- systemic inflammation
- plasma volume expansion
- microvascular dysfunction
- myocardial hypertrophy and fibrosis
- impaired ventricular relaxation
This model helps explain why the syndrome so often travels with obesity, insulin resistance, fatty liver, and sleep apnea, and why therapies that improve adiposity and metabolic biology may improve HFpEF.
The liver connection and the cardio-hepatic-metabolic axis
HFpEF frequently coexists with fatty liver disease and insulin resistance. That is not surprising. In the setting of excess nutrient exposure—especially refined carbohydrate and fructose—the liver becomes a major site of de novo lipogenesis, triglyceride overproduction, and metabolic dysregulation. The downstream effects include:
- elevated triglycerides
- worsening insulin resistance
- visceral fat expansion
- increased inflammatory signaling
This creates what can reasonably be described as a cardio-hepatic-metabolic axis, in which liver fat, visceral adiposity, and vascular dysfunction reinforce the cardiac phenotype. While HFpEF is not reducible to liver disease, many patients with obesity-related HFpEF are clearly living within the same metabolic environment that drives MASLD and metabolic syndrome. The adipokine-focused literature increasingly supports this integrated view.
Fructose, uric acid, and metabolic overload
Fructose is not the only cause of HFpEF, and it would be incorrect to present it as such. But it fits plausibly into the broader biologic pathway. High fructose exposure can promote:
- hepatic ATP depletion
- uric acid generation
- liver fat accumulation
- elevated triglycerides
- insulin resistance
- visceral fat expansion
These changes are compatible with the adiposity-driven and liver-centered models of HFpEF now being discussed in the literature. In that sense, fructose is best viewed as an important upstream contributor to the metabolic environment in which HFpEF develops, particularly in obesity-related phenotypes.
Hypertension still matters
None of this replaces the importance of hypertension. Elevated blood pressure remains one of the strongest contributors to HFpEF because it promotes:
- concentric remodeling
- ventricular hypertrophy
- impaired relaxation
- elevated filling pressures
But in many patients today, hypertension is embedded in a broader syndrome that includes obesity, insulin resistance, sleep apnea, and visceral adiposity. That is why a purely blood-pressure-centered model is too narrow for many modern HFpEF patients. ACC guidance recommends aggressive control of blood pressure, generally to <130 mm Hg systolic when tolerated, as part of HFpEF care.
Sleep apnea and HFpEF
Sleep apnea is common in HFpEF and contributes through:
- intermittent hypoxia
- sympathetic activation
- worse blood pressure control
- increased cardiometabolic stress
This is one reason sleep apnea is specifically listed among the core comorbidities requiring active management in HFpEF. In practical terms, untreated sleep apnea can worsen the entire cardiometabolic phenotype.
Therapeutic implications: why modern therapies work
The modern therapeutic story of HFpEF makes more sense when viewed through a cardiometabolic lens.
Guideline-based therapy
ACC guidance supports treatment of comorbidities plus evidence-based heart failure therapies, with SGLT2 inhibitors now an important component of management for many patients with HFpEF. Blood pressure control, volume management, rhythm control where relevant, and treatment of obesity, diabetes, and sleep apnea all remain central.
Anti-obesity and incretin-based therapy
This is where the field has changed most dramatically. In the STEP-HFpEF program, semaglutide improved symptoms, physical limitations, and exercise capacity in obesity-related HFpEF. In the SUMMIT trial, tirzepatide reduced the risk of worsening heart-failure events or cardiovascular death and improved health status in patients with HFpEF and obesity.
Structural evidence
The story goes beyond weight loss alone. A 2024 JACC report from the SUMMIT CMR substudy showed that tirzepatide reduced left ventricular mass and paracardiac adipose tissue, directly supporting the concept that modifying pathologic fat depots can improve the HFpEF substrate itself.
In other words, for many patients with obesity-related HFpEF, treatment is increasingly about reversing metabolic and adipose-driven stress on the heart, not just relieving congestion.
Clinical message
The most clinically useful way to think about HFpEF today is this:
HFpEF is often the cardiovascular expression of a broader disorder involving:
- visceral obesity
- insulin resistance
- fatty liver
- inflammation
- endothelial dysfunction
- hypertension
- sleep apnea
This is why it belongs in the metabolic disease section of your site rather than being treated as a purely cardiology topic.
Bottom line
HFpEF is a major modern heart-failure syndrome, but it is often best understood as a cardiometabolic disease with cardiac manifestation. The preserved ejection fraction can be misleading; the deeper problem is often one of stiffness, congestion, microvascular dysfunction, abnormal fat biology, and systemic metabolic stress.
Current research increasingly supports a model in which visceral and epicardial adiposity, altered adipokines, insulin resistance, and liver-centered metabolic overload are central drivers of many HFpEF phenotypes. That is why modern treatment increasingly works by addressing the metabolic environment itself—not just by treating fluid retention after the fact.
Related pages
Metabolic Syndrome
Visceral Obesity
Hypertension
Sleep Apnea
Fatty Liver Disease (MASLD)
Fructose Metabolism
Uric Acid
Cardio-Hepatic Axis
Cardiovascular Disease