Introduction
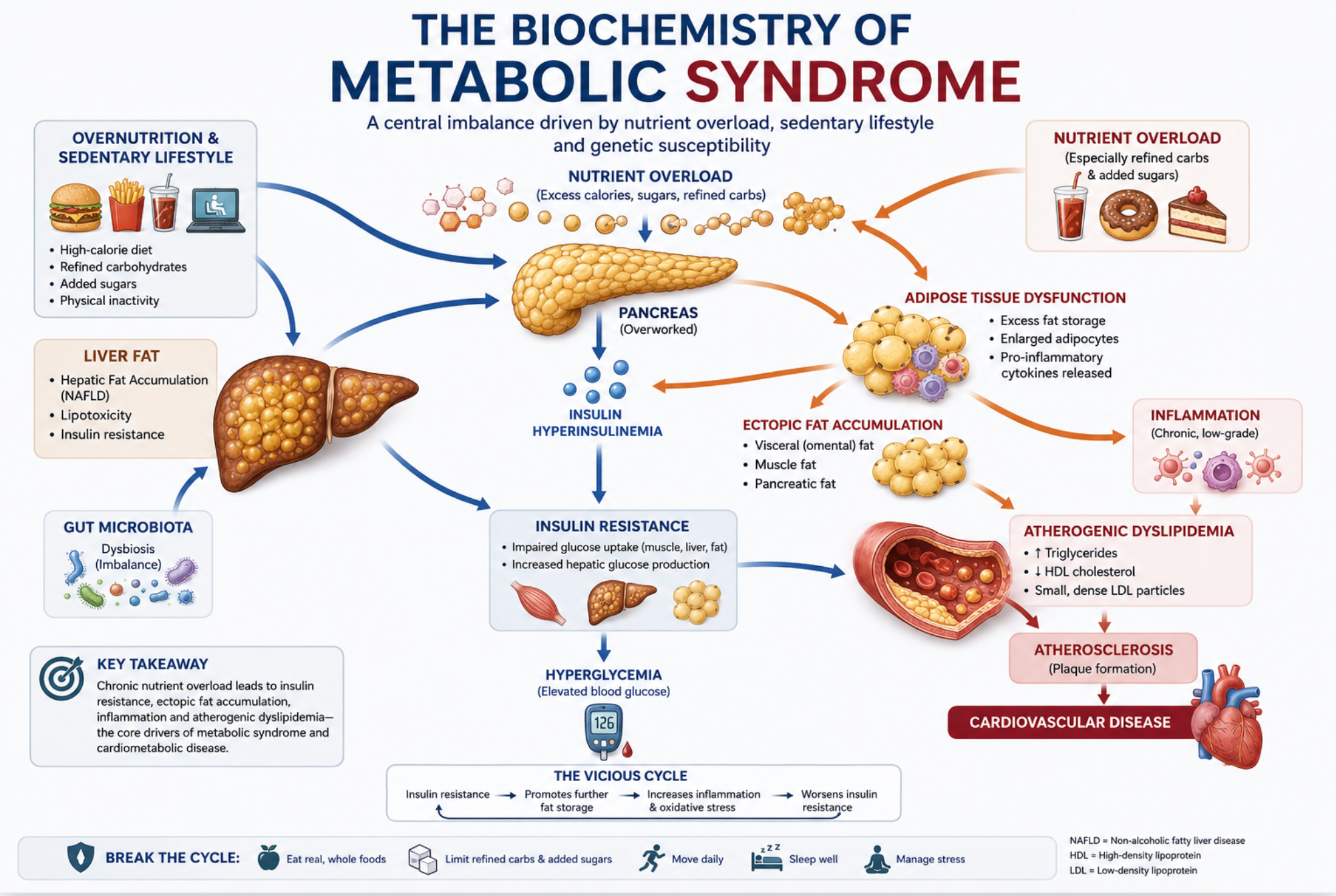
Metabolic syndrome is not a single disease. It is a pattern of biochemical overload affecting multiple organs that regulate energy, glucose, and lipid metabolism.
What appears clinically as obesity, elevated glucose, fatty liver, and abnormal lipids reflects a deeper internal process: chronic exposure to excess nutrient substrate.
Metabolic flexibility—and its loss
Normal metabolism is flexible.
The body can switch between:
- storing energy after meals
- mobilizing energy during fasting
This balance depends on coordinated signaling between liver, muscle, adipose tissue, and pancreas.
Metabolic syndrome begins when that flexibility is lost.
Metabolic overload
The central driver is metabolic overload.
When nutrient intake repeatedly exceeds the body’s capacity to process it:
- excess substrate accumulates
- storage pathways become saturated
- regulatory signaling begins to fail
Key early changes include:
- visceral fat expansion
- increased fatty acid flux to the liver
- rising triglyceride production
- early insulin resistance
This is not a single event—it is a sustained biochemical state.
The liver: central processing failure
The liver is the primary metabolic hub.
It receives nutrients directly from the intestine and regulates:
- glucose output
- lipid synthesis
- triglyceride export
Under chronic overload:
- fat accumulates in hepatocytes
- de novo lipogenesis increases
- VLDL production rises
- hepatic insulin signaling deteriorates
Fatty liver (MASLD) is often the first visible sign of this process.
De novo lipogenesis
Excess carbohydrate—especially fructose—is converted to fat in the liver.
This pathway is upregulated in metabolic syndrome:
- glucose and fructose enter hepatocytes
- acetyl-CoA is diverted into fatty acid synthesis
- triglycerides accumulate
- fat is exported as VLDL
This links dietary sugar directly to fatty liver and elevated triglycerides.
Visceral adipose tissue
Visceral fat is metabolically active.
As it expands, it releases:
- free fatty acids
- inflammatory cytokines
- adipokine signals that impair insulin action
This creates a feedback loop:
visceral fat expansion
→ inflammatory signaling
→ worsening insulin resistance
→ increased hepatic fat
Central obesity is therefore a biochemical driver, not just a marker.
Insulin resistance
Insulin resistance affects multiple tissues simultaneously.
- muscle takes up less glucose
- liver continues producing glucose
- pancreas increases insulin output
This leads to:
- hyperinsulinemia
- rising fasting glucose
- eventual pancreatic strain
Insulin resistance is both a consequence and amplifier of metabolic overload.
Triglycerides and lipid dysfunction
Metabolic syndrome produces a characteristic lipid pattern:
- elevated triglycerides
- reduced HDL cholesterol
- small, dense LDL particles
This reflects:
- hepatic overproduction of triglyceride-rich lipoproteins
- impaired lipid clearance
- altered lipoprotein remodeling
This pattern is strongly associated with cardiovascular risk.
Inflammation and vascular effects
Chronic metabolic overload produces low-grade inflammation.
This affects:
- adipose tissue
- liver
- vascular endothelium
Over time, this contributes to:
- endothelial dysfunction
- impaired vascular signaling
- atherosclerotic progression
Metabolic syndrome is therefore both a metabolic and vascular condition.
Why these abnormalities cluster
The defining feature of metabolic syndrome is clustering.
This occurs because the same underlying processes affect multiple organs:
- liver fat accumulation
- visceral adipose signaling
- insulin resistance
- triglyceride overproduction
- inflammatory activation
These are not separate diseases—they are interconnected expressions of the same biochemical state.
The modern food environment
Modern diets continuously drive these pathways.
Refined carbohydrates, added sugars, and ultra-processed foods:
- deliver rapid substrate
- lack fiber and satiety
- are consumed frequently throughout the day
This produces sustained metabolic pressure on the liver, pancreas, and adipose tissue.
Bottom line
Metabolic syndrome is the biochemical consequence of chronic overload of added sugars in the modern diet.
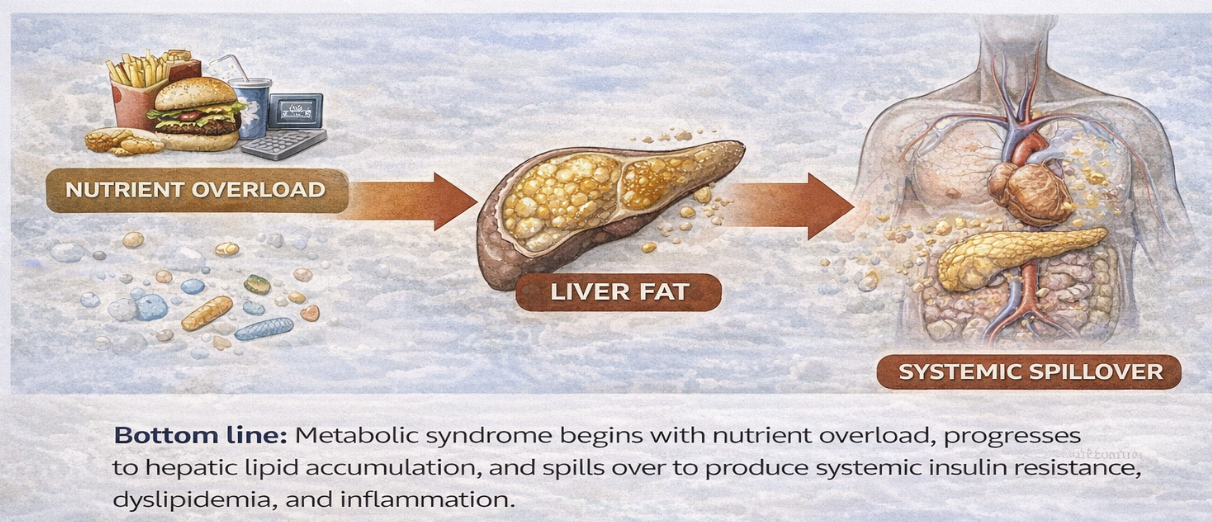
At its core are:
- excess nutrient exposure
- hepatic fat accumulation
- de novo lipogenesis
- visceral adipose signaling
- insulin resistance
- triglyceride overproduction
- low-grade inflammation
These processes interact across organs and over time, producing the clinical pattern recognized as metabolic syndrome.
Where to Go Next
Readers interested in exploring these topics further may wish to continue with the following sections:
• Fructose Metabolism
• Metabolic Syndrome
• Fatty Liver Disease (MASLD)
• Gene–Diet Interaction
Each of these topics examines a different aspect of the metabolic processes discussed in this overview.