Why Deep Abdominal Fat Matters
Not all body fat has the same biological effects. While subcutaneous fat is stored beneath the skin, another form of adipose tissue accumulates deep within the abdominal cavity around internal organs. This type of fat is known as visceral adipose tissue, or visceral fat.
Visceral fat is now recognized as one of the most important drivers of metabolic disease. Elevated visceral adiposity is strongly associated with:
- insulin resistance
- fatty liver disease
- metabolic syndrome
- Type 2 diabetes
- hypertension
- cardiovascular disease
This helps explain why body fat distribution often matters as much as, or more than, total body weight.

Types of Body Fat
Human adipose tissue exists in several forms, each with different physiological roles.
Subcutaneous fat
Subcutaneous fat is located beneath the skin and represents the majority of body fat in most individuals. Although excess subcutaneous fat can contribute to obesity, it is generally less metabolically harmful than visceral fat.
Visceral fat
Visceral fat surrounds organs within the abdominal cavity, including the liver, pancreas, and intestines. Because of its location and metabolic activity, it has a much stronger association with metabolic disease.
Ectopic fat
A third important category is ectopic fat, meaning fat stored in places where it does not normally belong, such as the liver, muscle, pancreas, or even around the heart. Ectopic fat often reflects more advanced metabolic dysfunction.
Adipose Tissue Is Not Just Storage
Adipose tissue was once viewed mainly as a passive storage site for excess energy. Modern research has shown that adipose tissue functions as an active endocrine and metabolic organ.
Fat tissue releases a wide range of signaling molecules known as adipokines, along with inflammatory mediators that influence:
- insulin sensitivity
- appetite regulation
- lipid metabolism
- immune responses
- vascular function
- systemic inflammation
This is especially true of visceral adipose tissue, which produces a more inflammatory and metabolically disruptive signaling profile than subcutaneous fat.
Why Visceral Fat Is So Dangerous
One reason visceral fat has such powerful metabolic effects is its direct relationship to the portal circulation.
Blood draining from visceral fat flows directly to the liver through the portal vein. This means that free fatty acids, adipokines, and inflammatory signals released from visceral fat reach the liver quickly and in relatively high concentrations.
This can influence several hepatic processes:
- lipid synthesis
- glucose regulation
- triglyceride production
- insulin sensitivity
- inflammatory signaling
Over time, this helps drive:
- fatty liver disease (MASLD)
- hypertriglyceridemia
- insulin resistance
- broader metabolic syndrome
Visceral Fat and Inflammatory Signaling
A central reason visceral fat is harmful is that it promotes chronic low-grade inflammation.
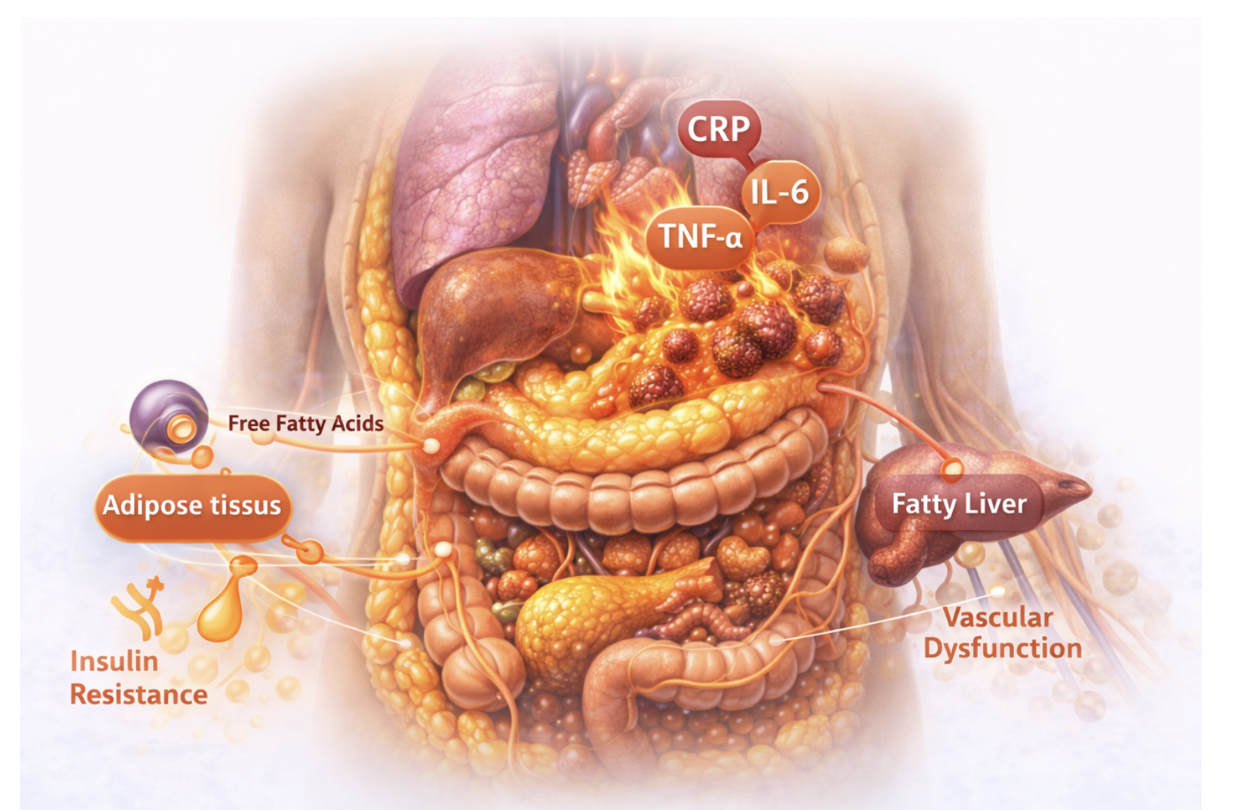
As visceral adipose tissue expands, it begins to release increased amounts of inflammatory signaling molecules, including:
- tumor necrosis factor-alpha (TNF-α)
- interleukin-6 (IL-6)
- monocyte chemoattractant protein-1 (MCP-1)
These cytokines interfere with normal metabolic regulation and help connect visceral fat to insulin resistance, liver dysfunction, and vascular disease.
Visceral fat therefore acts not just as stored energy, but as a biologically active source of inflammatory stress.
Immune Cells in Adipose Tissue
As visceral fat enlarges, immune cells begin to accumulate within it.
Macrophages and other immune cells are recruited into stressed adipose tissue and produce additional inflammatory mediators. This creates a self-reinforcing cycle:
visceral fat expansion → immune cell infiltration → more inflammation → worsening metabolic dysfunction
This process helps explain why visceral adiposity is so strongly linked to chronic metabolic disease.
Effects on Insulin Signaling
Visceral adiposity is strongly associated with insulin resistance.
Free fatty acids released from visceral fat can impair insulin action in the liver and muscle. At the same time, inflammatory cytokines such as TNF and IL-6 can disrupt the normal intracellular pathways that allow cells to respond to insulin.
As insulin sensitivity declines:
- the pancreas must produce more insulin
- blood glucose regulation becomes less stable
- liver fat tends to increase
- triglycerides often rise
Over time, this contributes to the development of:
- metabolic syndrome
- prediabetes
- Type 2 diabetes
Interaction With Liver Metabolism
Because visceral fat drains directly into the portal vein, it has especially strong effects on the liver.
Fatty acids and inflammatory signals from visceral adipose tissue can promote:
- hepatic lipid synthesis
- increased glucose production
- insulin resistance
- triglyceride overproduction
- progression toward MASLD
This is why visceral adiposity and fatty liver disease are so closely linked.
In many patients, visceral fat is one of the clearest external clues to liver-centered metabolic dysfunction.
Cardiovascular Implications
Visceral fat also affects the cardiovascular system.
Inflammatory mediators and altered metabolic signals from visceral adipose tissue may contribute to:
- endothelial dysfunction
- vascular inflammation
- hypertension
- atherosclerosis
- broader cardiometabolic disease
This helps explain why central obesity is so strongly associated with cardiovascular risk even when overall body size does not fully capture the severity of metabolic disease.
Measuring Visceral Fat
The most direct way to measure visceral fat is through imaging, especially:
- CT scanning
- MRI
In routine clinical practice, however, simpler surrogate markers are often used.
Common practical markers include:
- waist circumference
- waist-to-height ratio
- central abdominal body shape
These measures do not directly quantify visceral fat, but they often provide useful clues about visceral adiposity and metabolic risk.
Visceral Fat in the Modern Environment
The global increase in obesity has been accompanied by a rise in visceral adiposity.
Contributors include:
- increased intake of refined carbohydrates and sugary drinks
- greater availability of energy-dense processed foods
- sedentary lifestyles
- reduced physical activity
- poor sleep
- chronic stress
These environmental pressures interact with genetic susceptibility and metabolic biology to shape where fat is stored and how damaging it becomes.
Improving Metabolic Health
One of the encouraging features of visceral fat is that it can decline with lifestyle and metabolic improvement, often even before dramatic total weight loss occurs.
Interventions that may help reduce visceral adiposity include:
- regular physical activity
- improved diet quality
- reduction of sugary beverages and ultra-processed foods
- improved sleep
- reduction of excess caloric intake
- treatment of insulin resistance and metabolic syndrome where appropriate
Reducing visceral fat may improve:
- insulin sensitivity
- liver fat
- triglycerides
- inflammatory burden
- cardiovascular risk
Why This Matters
Visceral adiposity helps explain why metabolic disease is not simply a matter of body size.
Two people may have similar body weight, but very different levels of metabolic risk depending on how much fat is stored viscerally and how active that fat is as an inflammatory organ.
This is why visceral fat is now viewed as one of the key biological links between:
- obesity
- insulin resistance
- fatty liver disease
- inflammation
- cardiovascular disease
Bottom Line
Visceral adiposity is more than excess abdominal fat. It is a biologically active, inflammatory, metabolically disruptive form of fat storage that plays a central role in modern metabolic disease.
Because visceral fat:
- drains directly to the liver
- releases inflammatory cytokines
- disrupts insulin signaling
- worsens lipid metabolism
- promotes vascular dysfunction
it helps drive the clustering of conditions seen in metabolic syndrome.
In practical terms, visceral fat is one of the clearest markers that metabolic overload is already underway.
Related Pages
- Metabolic Syndrome
- Insulin Resistance
- Fatty Liver Disease (MASLD)
- Inflammation
- TNF
- Interleukin-6
- Adiponectin
- Cardio-Hepatic Axis
- Type 2 Diabetes