A Disorder of Breathing, Sleep, and Metabolic Stress
What is sleep apnea?
Sleep apnea is a condition in which breathing repeatedly stops or becomes abnormal during sleep.
There are two main types:
- Obstructive sleep apnea (OSA) — caused by collapse or narrowing of the upper airway
- Central sleep apnea (CSA) — caused by disrupted signals from the brain that control breathing
Both forms interfere with normal oxygen delivery and sleep quality, but they arise from different mechanisms.
Obstructive vs central sleep apnea
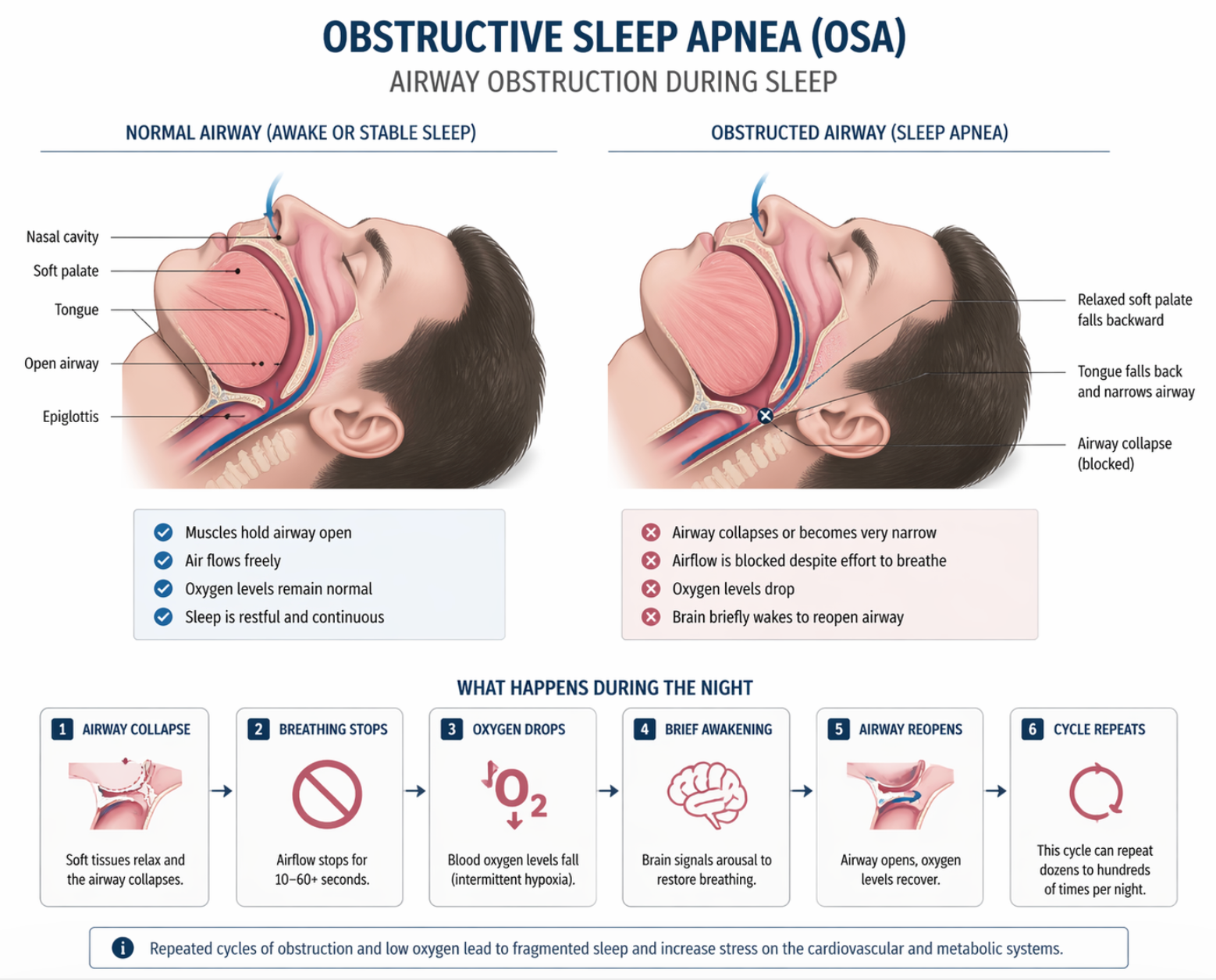
Obstructive sleep apnea (OSA)
This is the most common form.
During sleep:
- the muscles that keep the airway open relax
- the airway narrows or collapses
- airflow is reduced or stops
- oxygen levels fall
The brain briefly wakes the person to restore breathing.
This cycle may occur:
- dozens to hundreds of times per night
Central sleep apnea (CSA)
In central sleep apnea:
- the airway is open
- but the brain fails to send consistent signals to breathe
This leads to:
- pauses in breathing
- irregular breathing patterns
- unstable oxygen levels
CSA is more commonly associated with:
- heart failure
- neurological conditions
- advanced metabolic and cardiovascular disease
What happens during an apnea event
Each episode triggers a cascade:
- oxygen levels drop
- carbon dioxide rises
- stress hormones increase
- the brain briefly arouses the body
These events are short, but repeated continuously throughout the night.
Fragmented sleep and oxygen stress
Sleep apnea creates two major physiological stresses:
1. Sleep fragmentation
- repeated awakenings
- reduced deep sleep
- impaired recovery
2. Intermittent hypoxia
- repeated drops in oxygen
- activation of stress pathways
- increased sympathetic nervous system activity
This combination affects the entire body.
Why sleep apnea is a metabolic disease
Sleep apnea is strongly linked to metabolic syndrome.
It is associated with:
- central obesity
- insulin resistance
- fatty liver disease (MASLD)
- elevated triglycerides
- hypertension
This is not coincidence.
👉 The same processes that drive metabolic disease also drive sleep apnea.
The role of fat distribution
Excess fat is not just stored under the skin.
It accumulates in critical locations:
- around the neck and airway
- in the tongue and soft tissues
- in visceral fat depots
This contributes to:
- airway narrowing
- increased collapse during sleep
At the same time, visceral fat produces inflammatory signals that worsen metabolic dysfunction.
Fructose, liver fat, and sleep apnea
The connection to diet is often overlooked.
High intake of refined carbohydrates and sugary beverages—especially those containing fructose—leads to:
- increased liver fat production
- elevated triglycerides
- visceral fat accumulation
- insulin resistance
These changes contribute to:
- airway fat deposition
- altered respiratory control
- increased risk of obstructive sleep apnea
👉 In this way, sleep apnea can be seen as part of the broader fructose-driven metabolic pathway.
Insulin resistance and breathing control
Insulin resistance affects more than glucose metabolism.
It is associated with:
- altered autonomic nervous system activity
- impaired respiratory regulation
- increased airway instability
These changes contribute to both:
- obstructive sleep apnea
- central sleep apnea in advanced disease
Cardiovascular and metabolic effects
Sleep apnea increases risk of:
- hypertension
- arrhythmias
- coronary artery disease
- stroke
- heart failure
Repeated hypoxia and stress activation lead to:
- vascular dysfunction
- inflammation
- increased cardiac workload
This places sleep apnea within the broader cardiometabolic disease spectrum.
Clinical presentation
Common features include:
- loud snoring
- pauses in breathing during sleep
- excessive daytime sleepiness
- morning headaches
- poor concentration
However, many patients do not recognize the condition.
Diagnosis
Sleep apnea is diagnosed with:
- overnight sleep studies (polysomnography)
- home sleep testing
Severity is measured by the apnea–hypopnea index (AHI).
Treatment
Treatment addresses both airway function and underlying metabolic factors.
Common approaches include:
- CPAP (continuous positive airway pressure)
- weight reduction
- oral appliances
- positional therapy
In some cases:
- treatment of heart failure or neurological conditions (for CSA)
Why weight loss matters
Weight loss improves:
- airway structure
- breathing stability
- metabolic function
This is why treatments that reduce body fat—especially visceral fat—often improve sleep apnea.
A broader metabolic framework
Sleep apnea is best understood as part of a larger system:
dietary excess → liver fat → visceral adiposity → insulin resistance → airway instability and metabolic disease
It is not just a sleep disorder.
It is a manifestation of systemic metabolic stress.
Bottom line
Sleep apnea reflects the interaction between:
- airway structure
- brain control of breathing
- metabolic health
Obstructive and central forms differ in mechanism, but both are influenced by the same underlying metabolic environment.
High sugar intake, liver fat, and visceral adiposity contribute to the development and progression of sleep apnea.
Treating sleep apnea improves symptoms, but addressing the underlying metabolic drivers is essential for long-term improvement.
Related pages
Metabolic Syndrome
Obesity / Central Obesity
Insulin Resistance
Type 2 Diabetes
Fatty Liver Disease
HFpEF