Evolution, Adaptation, and the Human Metabolic Story
Survival begins with food
For any species, the first biological challenge is survival.
That means finding food, using it efficiently, and living long enough to reproduce.
In Darwinian terms, individuals best matched to their environment are more likely to survive and pass on their traits. Food is central to that process.
If a population lives for generations in an environment where the available foods are roots, grains, marine fats, seasonal fruit, or animal foods, then traits that help handle those foods may become more common over time.
This is how food environment and biology become linked.
Food environments shape adaptation
Human beings did not evolve in one global food system.
They evolved in very different food environments, including:
- tropical forests
- arctic coastlines
- islands
- grasslands
- deserts
- river valleys
- mountain regions
Each environment favored different dietary patterns.
Some populations depended heavily on:
- root crops
- grains and legumes
- fish and marine foods
- animal fat and protein
- seasonal fruits
- fermented foods
Over thousands of years, this shaped differences in how food was:
- digested
- stored
- used for energy
- converted into fat
Adaptation is not only about climate. It is also about food.
Dietary adaptation matters as much as other adaptations
When people think of human adaptation, they often think of:
- altitude
- climate
- skin pigmentation
- cold or heat tolerance
But dietary adaptation is just as important.
Food is one of the most persistent selective pressures in human life. A population repeatedly exposed to a certain food pattern may gradually favor traits that help with:
- starch handling
- fat metabolism
- insulin response
- uric acid handling
- energy storage
- dairy digestion
These adaptations do not make one group “better” than another. They make populations better matched to the historical foods of their environment.
From adaptation to mismatch
In traditional settings, efficient energy storage could be protective.
Traits that favor:
- rapid fat storage
- conservation of energy
- strong lipogenic response
- survival during scarcity
may improve survival where food is seasonal or unpredictable.
In those settings, storing energy efficiently is not a disease trait. It is an advantage.
The problem appears when the environment changes but the underlying biology does not.
Modern food systems now provide:
- constant food availability
- refined carbohydrates
- sugary beverages
- ultra-processed foods
- frequent eating
This creates a mismatch.
Genes shaped by older environments are now exposed to a food system they were never selected to manage.
Key genes and why they matter
Not every metabolic difference between populations is genetic, and genes are never destiny. But some genes and gene clusters repeatedly appear in research because they help explain why people differ in how they handle starch, dairy, fructose, fat, liver fat accumulation, and uric acid. What matters clinically is not one gene in isolation, but how these genes interact with a modern industrial food environment.
AMY1
Starch digestion
What it does
AMY1 influences salivary amylase production, which begins starch digestion in the mouth. Higher AMY1 copy number is generally associated with higher salivary amylase levels.
Why it matters
It helps explain why some populations appear better adapted to long histories of starch-rich diets.
Populations often discussed
- East Asian populations with long starch-rich agricultural histories
- Mediterranean agricultural populations
- lower-starch historical populations are often discussed as a contrast, though AMY1 is only part of the story
Clinical implications
AMY1 may influence post-meal glucose response, but it does not make ultra-refined starch harmless. Even high-AMY1 populations can still develop insulin resistance when exposed to instant starches, refined flour, and continuous snacking.
LCT
Dairy digestion and lactase persistence
What it does
LCT and nearby regulatory variants influence whether lactase activity persists into adulthood. Lactase persistence is common in populations with long histories of dairying and much less common in many East Asian, Indigenous American, and some Southeast Asian populations. It also evolved independently in some African and Middle Eastern pastoralist groups.
Why it matters
This is one of the clearest examples of human dietary adaptation.
Populations often discussed
- Northern Europeans
- some East African pastoralist groups
- some Middle Eastern pastoralist groups
- lower persistence in many East Asians, Indigenous Americans, and parts of Southeast Asia
Clinical implications
Lactase persistence may support tolerance of milk in adulthood. Low persistence makes lactose intolerance more likely, and fermented dairy is often tolerated better than liquid milk.
FADS gene cluster
Fat handling and long-chain fatty acid metabolism
What it does
The FADS1/FADS2 cluster helps regulate conversion of shorter-chain dietary fatty acids into longer-chain polyunsaturated fatty acids. Variation in this region has been under dietary selection in different populations.
Why it matters
It may influence how populations respond to plant-heavy fat intake versus direct intake of marine or animal sources of long-chain fats.
Populations often discussed
- European populations across agricultural transitions
- African-descent and Hispanic/Latino populations in whom FADS-related interactions with modern fat intake have been studied
- Arctic and marine-food populations are often discussed in contrast, though multiple genes are involved
Clinical implications
FADS variation may help explain differences in inflammatory lipid patterns and responses to diets high in seed oils or low in marine fats.
TCF7L2
One of the strongest Type 2 diabetes genes
What it does
TCF7L2 is one of the most consistently replicated genetic associations in Type 2 diabetes. It appears to influence insulin secretion and beta-cell function more than obesity itself.
Why it matters
This helps explain why some populations develop diabetes early, sometimes even without extreme obesity.
Populations often discussed
- widely replicated across European, South Asian, East Asian, Middle Eastern, African-descent, and Hispanic populations
Clinical implications
TCF7L2 helps explain early progression from insulin resistance to overt diabetes in susceptible individuals.
FTO
Obesity, appetite, and visceral fat risk
What it does
FTO is one of the best-known obesity-associated genes. It is linked to higher BMI and increased obesity risk, especially in calorie-dense food environments.
Why it matters
It helps explain why some people are more prone to weight gain and visceral adiposity under ultra-processed, high-calorie modern diets.
Populations often discussed
- broad relevance across multiple populations, including European, African-descent, Middle Eastern, South Asian, and Latin American groups
Clinical implications
FTO does not “cause obesity,” but it can amplify risk in a food environment dominated by refined carbohydrates, sugary drinks, and frequent intake.
SLC2A9 / GLUT9 and ABCG2
Uric acid handling, gout, and kidney risk
What they do
These genes are involved in uric acid transport and excretion. Variation in them can influence how efficiently the body clears uric acid.
Why they matter
They help explain why some populations are more vulnerable to:
- hyperuricemia
- gout
- kidney stone risk
- uric-acid–linked hypertension and kidney disease
especially when modern diets include high fructose exposure.
Populations often discussed
- Polynesian and Pacific populations
- African-descent populations
- Southeast Asian populations
- broader relevance across many populations, with prevalence varying by ancestry and study population
Clinical implications
These genes are especially important in the modern era because fructose can increase uric acid production, making poor excretion more clinically significant.
KHK and GLUT5
Fructose handling
What they do
- GLUT5 helps transport fructose across the intestinal wall
- KHK, or ketohexokinase, drives rapid fructose phosphorylation in the liver
Why they matter
These are central to the mechanism of fructose toxicity. In a high-sugar environment, they help explain:
- ATP depletion
- uric acid generation
- liver fat production
- de novo lipogenesis
- triglyceride elevation
Clinical implications
These genes matter because they sit at the center of the fructose → liver → uric acid → fat pathway, even if population-level polymorphism effects are less clinically settled than for LCT or TCF7L2.
👉 See: Fructose Metabolism
PNPLA3
Liver fat and steatotic liver disease
What it does
PNPLA3 is one of the most important genes in fatty liver disease. The rs738409 variant is strongly associated with hepatic fat accumulation and more severe steatotic liver disease.
Why it matters
This is one of the clearest examples of a gene that connects diet, liver fat, and downstream metabolic disease.
Populations often discussed
- particularly relevant in Hispanic/Latino populations, where the risk variant is more common and contributes to higher fatty liver burden
- also important across many other populations, but the population distribution is not uniform
Clinical implications
PNPLA3 helps explain why some people develop fatty liver and its complications more readily, especially under high-fructose, high-sugar conditions.
CREBRF
Pacific populations and efficient energy storage
What it does
The CREBRF rs373863828 variant is one of the most discussed population-specific metabolic variants. It is common in Polynesian populations and has been associated with higher BMI, with a more complex relationship to diabetes risk.
Why it matters
It is one of the strongest modern examples of a potential efficient-energy-storage adaptation.
Populations often discussed
- Polynesian populations
- Māori and other Pacific peoples
- broader Pacific populations in the Pacific Islands literature
Clinical implications
CREBRF helps explain why some Pacific populations may show extreme obesity risk in modern food environments, even though the diabetes relationship is more nuanced than a simple one-gene explanation.
What diseases do these genes help explain?
These genes help explain why populations may differ in susceptibility to:
- rapid post-meal glucose spikes and hyperinsulinemia
- visceral obesity
- fatty liver disease (MASLD)
- hypertriglyceridemia
- hyperuricemia and gout
- Type 2 diabetes at lower BMI
- hypertension and kidney disease in the setting of uric acid and metabolic overload
The genes do not create disease by themselves. The disease emerges when inherited biology collides with a new food environment.
Ethnic variability in handling food
This is where population differences become clinically relevant.
Different groups may vary in:
- starch digestion
- insulin response
- fat storage patterns
- liver fat susceptibility
- uric acid handling
- metabolic syndrome risk at lower or higher body weight
Examples across this site include:
- Pacific populations with strong energy-storage traits
- Indigenous North American populations with high vulnerability after rapid dietary disruption
- East Asian populations who may develop metabolic disease at lower BMI
- Arctic populations historically adapted to marine foods
- Mesoamerican and Andean populations adapted to maize- or root-based systems
These are not random differences. They reflect long interaction between genes and food environment.
Food structure matters too
Adaptation is not only about ingredients.
It is also about how food is eaten.
Traditional diets often included:
- defined meals
- lower sugar exposure
- slower digestion
- more fiber
- fewer liquid calories
The structure of the diet mattered as much as the nutrients themselves.
Modern diets disrupt both:
- the type of food
- the pattern of eating
Fructose as a modern stressor
One of the biggest changes in the modern diet is the rise of concentrated sugar, especially fructose in processed foods and beverages.
Historically, fructose exposure was:
- limited
- seasonal
- buffered within whole fruit
Now it is:
- frequent
- concentrated
- rapidly absorbed
- delivered in liquid form
This matters because fructose is handled primarily by the liver and may amplify:
- liver fat
- triglycerides
- insulin resistance
- uric acid production
In genetically susceptible populations, this can accelerate metabolic disease.
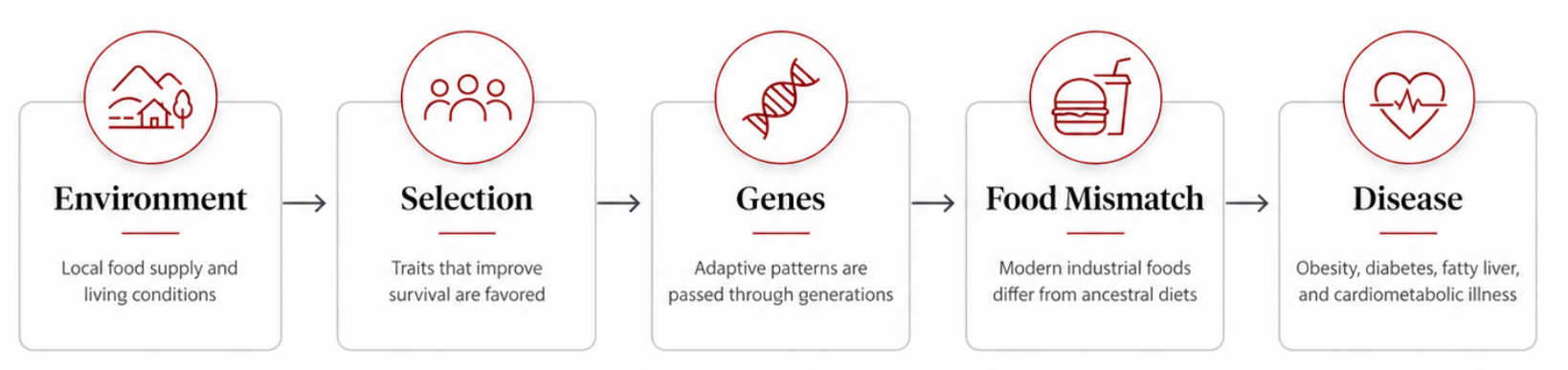
The global pattern
Across the world, the same sequence appears:
traditional food environment
→ adaptation over generations
→ rapid introduction of modern industrial foods
→ mismatch
→ metabolic disease
The visible disease differs by region, but the underlying logic is the same.
Why this matters clinically
This page is not about biological determinism.
It does not mean genes are destiny.
It means populations may begin from different metabolic starting points, and the same modern food environment can produce:
- different speeds of disease onset
- different severity
- different dominant syndromes
This helps explain why:
- some groups develop diabetes early
- some develop fatty liver at lower weight
- some show stronger uric acid responses
- some tolerate older food systems better than modern diets
Bottom line
Human beings adapted over thousands of years to the foods available in their local environments.
The most useful genes to discuss clinically are the ones that help explain major modern disease patterns:
- AMY1 → starch handling
- LCT → dairy tolerance
- FADS → fat metabolism
- TCF7L2 → diabetes risk
- FTO → obesity and adiposity
- SLC2A9 / ABCG2 → uric acid handling
- KHK / GLUT5 → fructose pathway
- PNPLA3 → fatty liver risk
- CREBRF → Pacific energy-storage phenotype
These do not act in isolation. But together, they help explain why the same modern food system produces different disease patterns across populations.
Related pages
Evolution and Diet
Ancestral Foods
Fructose Metabolism
GLUT5
Global Metabolic Transition
Indigenous North America
Pacific Islands
East Asia